Introduction
If you take Ozempic and are thinking about stopping, you are not alone. The cost, the weekly injections, the side effects, or just the desire to “do it on your own”, these are all common reasons people consider quitting. But what actually happens when you stop?
Ozempic (semaglutide) is a GLP-1 receptor agonist. It works by mimicking a hormone your gut naturally produces, one that tells your brain you are full and tells your pancreas to release insulin. When you take it away, those signals change. Understanding what that means for your body, your weight, and your appetite makes the difference between an informed decision and a rough surprise.
Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Do not stop or change any medication without consulting your healthcare provider. Abrupt discontinuation of Ozempic can have health consequences, especially if you have type 2 diabetes.
What The STEP 1 extension trial found
The most important study on this question comes from the STEP 1 trial extension, published in 2022 by Wilding and colleagues PMID: 35441470. In the original STEP 1 trial, participants without diabetes lost a mean of 17.3% of their body weight over 68 weeks on semaglutide 2.4 mg weekly PMID: 33567185. That is a lot, roughly 40 pounds for a 230-pound person.
Then they stopped the medication. Researchers followed participants for another 52 weeks with no semaglutide, though everyone continued receiving lifestyle counseling. Here is what happened: by week 120, participants had regained roughly two-thirds of the weight they lost. Their net weight loss from baseline dropped to about 5.6%, still something, but a fraction of the peak result.
The cardiometabolic improvements reversed too. Blood pressure crept back up. HbA1c returned toward baseline. Waist circumference expanded again. The drug had been doing real physiological work, and when it was removed, the body’s underlying biology reasserted itself.
The STEP 4 trial told a similar story from a different angle. After a 20-week run-in period where everyone took semaglutide and lost about 10.6% of body weight, researchers randomized participants to either continue the drug or switch to placebo. Over the next 48 weeks, the semaglutide group lost another 7.9%. The placebo group regained 6.9%, ending up near where they started PMID: 33755728.
Why Weight comes back
A 2026 systematic review and nonlinear meta-regression by Budini and colleagues mapped out the trajectory of weight regain after GLP-1 receptor agonist cessation PMID: 41938838. The pattern they found was not a slow creep. It was a rapid rebound in the first few months, followed by a gradual leveling off. This matches what most patients describe.
The biology behind this is well understood. GLP-1 receptor agonists suppress appetite by acting on receptors in the hypothalamus and by slowing gastric emptying. When you stop the drug, both effects disappear within days to weeks. Your stomach empties faster. The satiety signals that kept you satisfied on smaller portions go quiet. Hunger hormones that the medication had been holding down come roaring back.
A 2025 systematic review and meta-analysis by Tzang and colleagues examined the metabolic rebound specifically PMID: 41399474. They documented that discontinuation leads to increases in body weight, waist circumference, blood pressure, and glycemic markers. The authors described it as a “metabolic rebound”, and the word rebound matters. This is not your body going back to normal. It is your body overcorrecting past normal, at least temporarily.
Another systematic review from Berg and colleagues, also published in 2025, confirmed these findings across multiple GLP-1 receptor agonists PMID: 40186344. Their meta-analysis showed consistent weight regain after discontinuation across liraglutide, semaglutide, and other agents in the class. The effect sizes were large and the direction was uniform.
Quimbayo-Cifuentes, writing in a 2026 editorial, reframed weight regain not as a treatment failure but as physiology doing what physiology does PMID: 41909366. He argued that calling this “failure” misunderstands what obesity is. Like hypertension, it is a chronic condition that requires ongoing management. You would not call it a failure if someone’s blood pressure went back up after stopping their antihypertensive.
Physical withdrawal effects
Ozempic does not cause the kind of withdrawal you associate with opioids or benzodiazepines. There is no acute withdrawal syndrome. But people do notice physical changes when they stop, and some of them can be uncomfortable.
Days 1 through 7: Appetite returns, often abruptly. Portions that felt impossible to finish suddenly seem reasonable again. Bowel habits change as gastric emptying speeds back up. Some people who had constipation on Ozempic experience loose stools or diarrhea during this window.
Weeks 2 through 4: The hunger intensifies. This is the period when people most often describe feeling out of control around food. Cravings for high-calorie, high-carbohydrate foods become more frequent. The “food noise” comes back, and for many, this is the hardest part.
Weeks 4 through 12: Weight regain begins. The scale starts moving upward, and it moves quickly. In the STEP 1 extension, the steepest regain occurred during this period. Energy levels can fluctuate as blood sugar patterns shift. People with type 2 diabetes may see their glucose readings climb. This requires medical monitoring and likely medication adjustments.
Beyond 3 months: The rate of regain slows but does not always stop. The body finds a new set point, but it is often higher than the weight people maintained on the medication.
A 2025 narrative review by Quarenghi and colleagues examined weight regain patterns across liraglutide, semaglutide, and tirzepatide PMID: 40507553. They found that while tirzepatide users regained somewhat less weight after stopping (likely because of the dual GIP/GLP-1 mechanism), the overall pattern was the same: weight comes back when the medication stops.
Psychological effects
For many people, the mental and emotional experience of stopping Ozempic is harder than the physical one.
A 2026 study by de Vere Hunt and colleagues published in JAMA Network Open examined patient experiences with GLP-1 receptor agonists PMID: 42247231. Patients described the return of “food noise” (the constant, intrusive thoughts about food that the medication had quieted) as one of the most distressing aspects of discontinuation. Many had not realized how loud that noise had been until the drug turned down the volume.
When the volume comes back up, it can feel overwhelming. People describe thinking about food all day. Planning the next meal while eating the current one. Feeling hungry even after a full meal. This is not a failure of willpower. It is the return of neurobiological signals that GLP-1 receptor agonists had been suppressing.
There is also the emotional weight of seeing the scale climb. After months of watching the number go down, watching it reverse direction can trigger feelings of shame, frustration, and hopelessness. Some people describe avoiding the scale entirely. Others obsess over it. Neither response is unusual.
The social dimension matters too. People who received compliments on their weight loss may feel embarrassed or exposed as the weight returns. If stopping was driven by insurance denials or cost barriers rather than medical choice, there is often anger mixed in with the disappointment.
How To taper safely
If you and your doctor decide that stopping is the right move, tapering is gentler on your body than quitting abruptly. There are no large randomized trials testing specific tapering protocols, but clinical experience and pharmacological principles point to a reasonable approach.
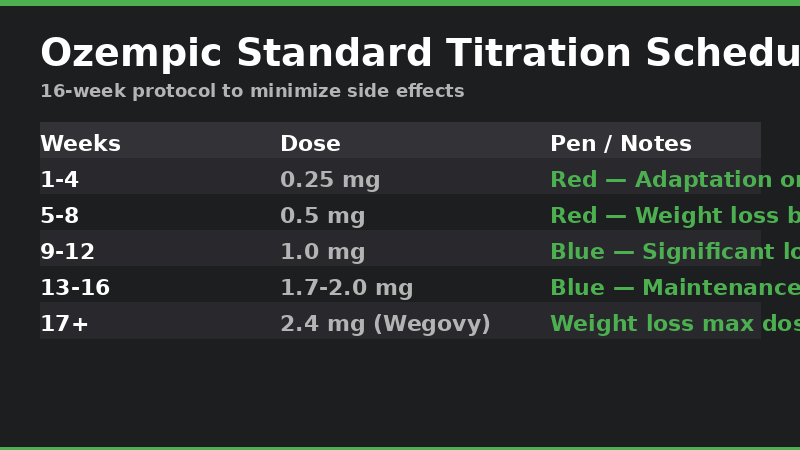
Step down through the doses in reverse. If you are at 2.4 mg weekly (the Wegovy maintenance dose), spend 4 weeks at 1.7 mg, then 4 weeks at 1.0 mg, then 4 weeks at 0.5 mg, then stop. If you are on the 1.0 mg or 2.0 mg Ozempic doses for diabetes, follow the same principle: drop one dose level every 4 weeks.
During each step-down, monitor your appetite, blood sugar (if you have diabetes), and weight. The goal is not to prevent all weight regain (that is unlikely). The goal is to prevent the jarring hunger surge that makes dietary adherence nearly impossible.
Do not taper without a doctor involved. If you take Ozempic for type 2 diabetes, stopping affects your glucose levels, and your other diabetes medications will likely need adjustment. A 2026 narrative review of nutritional priorities for GLP-1 therapy emphasized that discontinuation should be part of a comprehensive plan, not an isolated event PMID: 40673264.
Do not treat tapering as a back door to “cycling”, stopping and restarting repeatedly to avoid side effects or save money. There is no evidence that this approach is safe or effective, and it may increase the risk of gastrointestinal side effects when you restart.
Strategies to maintain weight loss after stopping
You cannot make your body forget that GLP-1 receptor agonists exist. But you can stack the odds in your favor. The evidence points to several strategies that help.
Protein intake matters more off the medication than on it. A 2026 review in Nutrients by Zambrano-Villacres and colleagues laid out a nutrition-first framework for supporting GLP-1 therapy and post-discontinuation maintenance PMID: 42280393. They recommended 1.2 to 1.6 grams of protein per kilogram of body weight daily, distributed across meals, to preserve lean mass and support satiety.
Resistance training helps in two ways. It preserves muscle that rapid weight loss can strip away. And it raises resting metabolic rate, modestly, yes, but every bit counts when your body’s appetite regulation is working against you. Aim for 2 to 3 sessions per week. Even bodyweight exercises are better than nothing.
Fiber is your friend. Soluble fiber, in particular, slows gastric emptying, mimicking a small fraction of what GLP-1 agonists do. Psyllium husk, oats, legumes, and chia seeds are all good sources. Start slow to avoid bloating and work up to 25 to 30 grams daily.
Sleep and stress management are not afterthoughts. Short sleep increases ghrelin (the hunger hormone) and decreases leptin (the satiety hormone). Chronic stress elevates cortisol, which promotes abdominal fat storage. If you are stopping Ozempic, getting 7 to 8 hours of sleep and having a stress management routine become part of the medical plan, not just wellness advice.
Consider whether another medication might help. Metformin, for example, has modest weight effects and is inexpensive. Some doctors prescribe it off-label for weight maintenance after GLP-1 discontinuation. Other options like bupropion/naltrexone (Contrave) or phentermine/topiramate (Qsymia) exist, but they have their own side effect profiles and limitations.
What you should not do is slash calories to try to compensate for the returning hunger. Very low-calorie diets after GLP-1 cessation risk muscle loss, nutrient deficiencies, and a metabolic adaptation that makes future weight loss even harder. Eat enough, prioritize protein, and accept that some regain is physiological, not a reflection of your effort.
Who Should not stop
For some people, stopping Ozempic carries risks that outweigh any potential benefit.
If you have type 2 diabetes, stopping means your blood glucose will rise. That is not a maybe. It is a certainty. The rise may be small or large depending on your baseline pancreatic function and what other medications you take. But it will happen. Uncontrolled hyperglycemia damages blood vessels, nerves, kidneys, and retinas over time. If your A1c was well-controlled on Ozempic, work with your doctor to have a replacement medication ready before you stop.
If you have obesity with significant weight-related comorbidities (sleep apnea, nonalcoholic fatty liver disease, osteoarthritis), the weight regain after discontinuation can worsen these conditions. Joints that felt better under less load will hurt again. Sleep apnea may return. Liver enzymes that normalized may climb back up.
If you have a history of binge eating disorder or severe food noise, stopping may trigger a relapse. The neurobiological suppression of food-related thoughts that GLP-1 agonists provide is not something you can replicate with willpower. Some people describe the return of food noise as more disabling than the original weight.
If you are stopping because of side effects, talk to your doctor about solutions before you decide to quit. Nausea often responds to dose adjustment, injection timing changes, or antiemetic medications. Constipation can be managed. Fatigue often improves after the first 8 to 12 weeks. Going down in dose is usually better than going off entirely.
Frequently asked questions
How long after stopping Ozempic does weight regain start?
Most people notice the scale moving within 2 to 4 weeks. The STEP 1 extension showed that regain begins quickly and is steepest in the first 3 to 6 months after discontinuation.
Can I stop Ozempic cold turkey?
You can, but tapering is easier on your body. Abrupt cessation means appetite and hunger signals return at full force overnight, which makes dietary control extremely difficult. If you take Ozempic for diabetes, stopping abruptly requires a plan for glucose management.
Will I gain back all the weight I lost?
On average, people regain about two-thirds of the weight they lost within one year, based on the STEP 1 extension data. Some people gain back everything. Some people retain a meaningful portion of their loss. Lifestyle factors (diet quality, exercise, sleep) influence where you land on that spectrum.
Is there a withdrawal syndrome from Ozempic?
No. Semaglutide and other GLP-1 receptor agonists do not cause a withdrawal syndrome in the medical sense. You will not experience cravings for the drug, physical dependence, or dangerous autonomic instability. What you will experience is the return of the appetite and metabolic patterns the drug had been suppressing.
Can I take Ozempic every other week instead of stopping?
Some doctors do prescribe extended-interval dosing, every 10 or 14 days instead of 7, as a maintenance strategy. However, semaglutide’s half-life is approximately one week, so extending the interval means the drug concentration in your body fluctuates more. There is limited published evidence on the efficacy of this approach. Discuss it with your doctor.
What happens if I stop and then restart later?
You would restart at the lowest dose (0.25 mg) and titrate back up over several months, just like when you first started. Do not restart at your previous high dose. This carries a real risk of severe gastrointestinal side effects including vomiting and pancreatitis.
Does weight regain happen with all GLP-1 medications?
Yes. The evidence is consistent across liraglutide (Saxenda), semaglutide (Ozempic, Wegovy), and tirzepatide (Mounjaro, Zepbound). Tirzepatide users may regain somewhat less because of the dual mechanism, but regain still occurs PMID: 40507553.
References
Wilding JPH, Batterham RL, Davies M, et al. Weight regain and cardiometabolic effects after withdrawal of semaglutide: The STEP 1 trial extension. Diabetes Obes Metab. 2022;24(8):1553-1564. PMID: 35441470
Rubino D, Abrahamsson N, Davies M, et al. Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial. JAMA. 2021;325(14):1414-1425. PMID: 33755728
Budini B, Luo S, Tam M, et al. Trajectory of weight regain after cessation of GLP-1 receptor agonists: a systematic review and nonlinear meta-regression. EClinicalMedicine. 2026;93:103796. PMID: 41938838
Tzang CC, Wu PH, Luo CA, et al. Metabolic rebound after GLP-1 receptor agonist discontinuation: a systematic review and meta-analysis. EClinicalMedicine. 2025;90:103680. PMID: 41399474
Berg S, Stickle H, Rose SJ, Nemec EC. Discontinuing glucagon-like peptide-1 receptor agonists and body habitus: A systematic review and meta-analysis. Obes Rev. 2025;26(8):e13929. PMID: 40186344
Quimbayo-Cifuentes AF. Weight Regain After GLP-1-Based Therapy Discontinuation: Failure, Physiology, or Follow-Up Gap. Cureus. 2026;18(2):e104259. PMID: 41909366
Quarenghi M, Capelli S, Galligani G, et al. Weight Regain After Liraglutide, Semaglutide or Tirzepatide Interruption: A Narrative Review of Randomized Studies. J Clin Med. 2025;14(11):3791. PMID: 40507553
de Vere Hunt I, Ramirez-Posada M, Babu CS, et al. Patient Experiences With GLP-1 Receptor Agonists. JAMA Netw Open. 2026;9(6):e2616951. PMID: 42247231
Mozaffarian D, Agarwal M, Aggarwal M, et al. Nutritional priorities to support GLP-1 therapy for obesity: A joint advisory from the American College of Lifestyle Medicine, the American Society for Nutrition, the Obesity Medicine Association, and the Obesity Society. Obes Pillars. 2025;15:100181. PMID: 40673264
Zambrano-Villacres R, Campuzano-Donoso M, Reytor-Gonzalez C, et al. Nutrition-First Support for GLP-1 and Dual Incretin Therapy in Obesity: A Practical Framework for Dietary Management, Symptom Tolerability, and Long-Term Weight Maintenance. Nutrients. 2026;18(11):1751. PMID: 42280393
Wilding JPH, Batterham RL, Calanna S, et al. Once-Weekly Semaglutide in Adults with Overweight or Obesity. N Engl J Med. 2021;384(11):989-1002. PMID: 33567185