Medical Disclaimer: This article is for informational purposes only and does not constitute medical advice. Ozempic (semaglutide) is a prescription medication FDA-approved for type 2 diabetes. Using it for weight loss without diabetes constitutes off-label use, which carries distinct risks and legal considerations. Do not start, stop, or change any medication without consulting a licensed healthcare provider. Weight loss medications carry risks including nausea, vomiting, pancreatitis, gallbladder disease, and thyroid C-cell tumors (observed in rodent studies; human relevance remains unconfirmed). Disclose your full medical history to your provider before pursuing any treatment.
Introduction
A neighbor of mine started Ozempic last spring. She doesn’t have diabetes , never has. Her A1c sits at 5.3, and her fasting glucose is textbook-perfect. But her BMI crossed 32 after two pregnancies and a desk job, and when her sister lost 40 pounds on the medication she figured, worth a shot. Her doctor agreed , with hesitation, and with a long conversation about what “off-label” actually means.
She’s not alone. A 2024 analysis of U.S. pharmacy claims found that roughly one in three Ozempic prescriptions now goes to patients without a type 2 diabetes diagnosis on file. That number was maybe one in ten back in 2020. The shift isn’t subtle, and it’s not happening in a regulatory vacuum, either. Novo Nordisk, Ozempic’s manufacturer, also sells Wegovy , chemically identical semaglutide, FDA-approved specifically for chronic weight management. And yet many non-diabetic patients still end up on Ozempic, either because their insurance dynamics push them there or because they simply don’t know there’s an alternative.
This guide unpacks the clinical evidence, the insurance trap, and the real-world experience of taking Ozempic for weight loss when you don’t have diabetes. Every section draws on published trial data, not marketing copy.
Ozempic vs Wegovy: what’s actually different?
Semaglutide is the active ingredient in both Ozempic and Wegovy. Chemically, it’s the same molecule , a GLP-1 receptor agonist that slows gastric emptying, suppresses appetite via hypothalamic signaling, and improves insulin secretion in a glucose-dependent manner. The difference between these two products has nothing to do with pharmacology and everything to do with regulatory labeling, dosing, and insurance architecture.
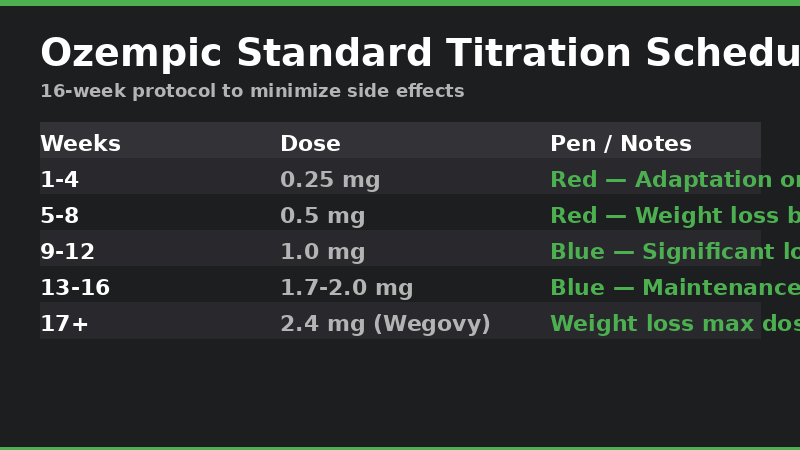
Ozempic is FDA-approved for type 2 diabetes. It comes in a multi-dose FlexTouch pen delivering 0.25 mg, 0.5 mg, 1.0 mg, or 2.0 mg per weekly injection. The 2.0 mg dose was added in 2022 after a phase 3 trial showed additional glycemic benefit; it also happens to deliver weight loss approaching what Wegovy achieves at 2.4 mg. That overlap is not accidental , it’s the same drug working through the same mechanism, and it’s exactly why physicians began prescribing it off-label for obesity before Wegovy hit the market.
Wegovy is FDA-approved for chronic weight management in adults with obesity (BMI ≥ 30) or overweight (BMI ≥ 27) with at least one weight-related comorbidity. It uses a fixed 2.4 mg weekly maintenance dose delivered via single-use autoinjector pens. The STEP clinical trial program, which enrolled over 5,000 participants across multiple studies, established that 2.4 mg semaglutide produces mean weight loss of roughly 15% of baseline body weight , a result that dwarfs earlier-generation obesity medications like orlistat (3–5%) or phentermine-topiramate (7–9%) [1].
The practical consequence of this labeling split is that Ozempic and Wegovy sit in entirely separate insurance coverage buckets. Ozempic falls under diabetes pharmacy benefits, where prior authorization criteria center on HbA1c and diagnosis codes. Wegovy falls under obesity benefits, which roughly 40% of large employer plans explicitly exclude. If your employer doesn’t cover weight loss drugs, Wegovy is $1,350 per month out of pocket, and Ozempic , covered or not , suddenly looks like the path of least resistance.
What the clinical trials say about non-diabetics
The evidence that semaglutide works for weight loss in non-diabetic populations is not circumstantial. It comes from a structured clinical development program that tested exactly this question.
STEP 1 (Wilding et al., NEJM 2021) enrolled 1,961 adults with overweight or obesity , and explicitly excluded those with diabetes. Participants on semaglutide 2.4 mg lost a mean of 14.9% of baseline body weight over 68 weeks compared to 2.4% with placebo. Nearly 86% of the semaglutide group lost at least 5% of body weight, and 69% lost at least 10% [1]. Those are not borderline results. They represent the largest weight loss ever reported in a pharmacotherapy trial for obesity at the time of publication.
STEP 3 (Wadden et al., JAMA 2021) added intensive behavioral therapy , 30 counseling sessions over 68 weeks , to the same 2.4 mg semaglutide dose in 611 participants without diabetes. The combination produced mean weight loss of 16.0%, compared to 5.7% with behavioral therapy plus placebo. What’s notable is that the behavioral therapy component added only about 1 percentage point to the STEP 1 result, suggesting semaglutide’s effect is robust with or without structured lifestyle support [2].
STEP 4 (Rubino et al., JAMA 2021) addressed the maintenance question: after 20 weeks of semaglutide run-in (during which participants lost a mean of 10.6% of body weight), those randomized to continue semaglutide for 48 more weeks lost an additional 7.9%, while those switched to placebo regained 6.9%. The net difference , nearly 15 percentage points , underlines a hard truth about GLP-1 therapy: it’s not a short-term fix. Stopping means regaining, and the trial data is unambiguous on this [3].
STEP 8 (Rubino et al., JAMA 2022) compared semaglutide 2.4 mg to liraglutide 3.0 mg (Saxenda, an older daily-injection GLP-1) in 338 adults without diabetes. Semaglutide produced mean weight loss of 15.8% versus 6.4% for liraglutide , more than double. The takeaway isn’t just that semaglutide works; it’s that not all GLP-1 agonists are interchangeable for weight loss, and the weekly formulation’s pharmacokinetic profile matters [4].
SELECT trial (Lincoff et al., NEJM 2023) enrolled 17,604 adults with preexisting cardiovascular disease, overweight or obesity, and no diabetes , by far the largest trial of semaglutide in a non-diabetic population. Over a mean follow-up of 39.8 months, semaglutide 2.4 mg reduced major adverse cardiovascular events (cardiovascular death, nonfatal MI, nonfatal stroke) by 20% compared to placebo. Mean weight loss at 2 years was 9.4% with semaglutide versus 0.9% with placebo [5]. This trial shifted the conversation from “can semaglutide help non-diabetics lose weight?” to “does semaglutide improve hard clinical outcomes in non-diabetics?” , and the answer is yes.
A 2026 meta-analysis published in the European Journal of Pharmacology pooled data from randomized controlled trials of semaglutide exclusively in non-diabetic adults with overweight or obesity. The analysis confirmed that semaglutide 2.4 mg produced consistent, clinically meaningful weight loss across all included studies, with a safety profile that mirrored what was observed in diabetic populations [6]. The evidence base for non-diabetic use is now large enough that the question has largely moved from “does it work?” to “how do we get it to the people who need it?”
How much weight Can you lose without diabetes?
The numbers from the STEP program tell a clear story, but clinical trial averages don’t always match what happens in the exam room. Trials have run-in periods, exclusion criteria, and adherence rates that real life rarely replicates.
Expected range for non-diabetics. Across the STEP trials that enrolled non-diabetic participants, mean weight loss on semaglutide 2.4 mg ranged from 14.9% (STEP 1, medication alone) to 16.0% (STEP 3, medication plus behavioral therapy) at 68 weeks [1][2]. In absolute terms, a 220-pound person can expect to lose roughly 30–35 pounds, though results vary considerably. About one in three participants in STEP 1 lost 20% or more of their body weight; about one in ten lost less than 5%.
Does having diabetes change the response? The short answer is yes, but the difference is smaller than many people assume. The STEP 2 trial enrolled participants with type 2 diabetes and found mean weight loss of 9.6% on semaglutide 2.4 mg , roughly 5 percentage points less than STEP 1’s non-diabetic cohort. The likely explanation involves insulin resistance, concurrent medications (some diabetes drugs promote weight gain), and differences in baseline metabolic function. Non-diabetic users tend to respond better, but the drug works in both groups [1].
What drives individual variation. Trial data and post-hoc analyses identify several factors associated with better response: female sex, lower baseline weight, and early weight loss trajectory. Participants who lost at least 5% of body weight by week 12 were far more likely to achieve ≥15% loss by week 68. The corollary , if you’re not seeing meaningful loss after 3–4 months at a therapeutic dose, semaglutide may not be the right drug for you , is worth discussing with your prescriber early.
The maintenance problem. STEP 4 demonstrated what happens when you stop: weight regain begins within weeks and continues steadily. At 1 year after discontinuing semaglutide, participants had regained roughly two-thirds of the weight they lost. This isn’t specific to semaglutide , it’s consistent with the broader obesity medicine literature showing that pharmacotherapy, like lifestyle intervention, requires ongoing treatment for durable effect. Obesity is a chronic condition, and treating it acutely produces acute results [3].
Is it safe? side effects in non-diabetic users
The side-effect conversation gets more complicated when you don’t have diabetes, because you’re accepting risk for a drug you don’t medically require. The calculus shifts.
Gastrointestinal effects dominate. In the STEP 1 trial, nausea occurred in 44% of semaglutide-treated participants versus 16% on placebo, diarrhea in 30% versus 16%, and vomiting in 25% versus 7%. Constipation and abdominal pain were also significantly more common. The majority of these events were mild to moderate in severity and transient , peaking during dose escalation and diminishing over weeks 8–20. About 7% of semaglutide-treated participants discontinued due to GI adverse events, compared to 3% in the placebo group [1].
Gallbladder disease. Rapid weight loss of any cause increases gallstone risk, and semaglutide-induced weight loss is no exception. Across the STEP program, cholelithiasis (gallstones) occurred in roughly 1–3% of semaglutide-treated participants versus less than 1% on placebo. Acute cholecystitis requiring surgical intervention was rare but reported. If you have a history of gallbladder problems, your prescriber needs to know before you start [1][3].
Pancreatitis. GLP-1 receptor agonists carry an FDA-mandated warning about acute pancreatitis, based on post-marketing reports and a plausible biological mechanism (GLP-1 receptors exist on pancreatic acinar cells). The absolute risk in clinical trials is low , typically less than 0.5% , but the consequences of pancreatitis are serious enough that any severe abdominal pain radiating to the back should trigger immediate medical evaluation. The risk does not appear to differ between diabetic and non-diabetic users [6].
Thyroid C-cell tumors. This is the black-box warning that scares people. In rodent studies, semaglutide caused dose-dependent and treatment-duration-dependent thyroid C-cell tumors at clinically relevant exposures. Whether this translates to humans is unknown , decades of GLP-1 agonist use have not produced a clear signal of elevated medullary thyroid carcinoma risk in post-marketing surveillance , but the FDA has not removed the warning. A personal or family history of medullary thyroid carcinoma or Multiple Endocrine Neoplasia syndrome type 2 (MEN2) remains an absolute contraindication.
Cardiovascular benefit. For non-diabetic patients with established cardiovascular disease or high cardiovascular risk, the risk-benefit calculus tilts toward favorability. The SELECT trial’s 20% reduction in major adverse cardiovascular events , a result comparable to what established cardioprotective drugs like statins and ACE inhibitors achieve in secondary prevention , suggests that for this subgroup, semaglutide may offer benefit beyond weight loss alone [5]. For young, otherwise healthy individuals taking the drug solely for weight loss, the equation is less clear, and a frank discussion with a physician about absolute versus relative risk is warranted.
The off-label prescription reality
Off-label prescribing is legal, common, and poorly understood by patients. In the United States, once the FDA approves a drug for any indication, licensed physicians may prescribe it for any condition they deem medically appropriate. Roughly one in five prescriptions written in the U.S. is off-label, and the practice is especially prevalent in psychiatry, oncology, and , increasingly , obesity medicine.
What “off-label” actually means. When a doctor writes Ozempic for a patient without diabetes, they are prescribing a drug for an indication the FDA has not formally evaluated and the manufacturer has not marketed. The legal authority to do this rests with the physician’s clinical judgment and is protected by the practice of medicine, which states , not the FDA , regulate. Novo Nordisk cannot promote Ozempic for weight loss, and they don’t. But physicians can prescribe it, and they do, in large and growing numbers.
Why prescribers choose Ozempic over Wegovy. The reasons are almost entirely financial, not medical. Wegovy’s list price and Ozempic’s list price are within $50 of each other at roughly $1,350 per month, but insurance coverage patterns differ dramatically. Commercial plans are far more likely to cover Ozempic , even with prior authorization , than Wegovy, because diabetes drugs fall under essential health benefits in a way that obesity drugs do not. A 2024 Kaiser Family Foundation analysis found that Medicare Part D plans cover Ozempic but are legally barred from covering Wegovy and other weight-loss medications, though legislative efforts to amend this prohibition continue. For patients whose insurance covers Ozempic with a diabetes diagnosis but won’t touch Wegovy, the off-label route is sometimes the only financially viable option.
The supply shortage complication. The FDA’s drug shortage database listed semaglutide injection as “currently in shortage” for much of 2023 and 2024 due to surging demand. During shortage periods, compounding pharmacies are legally permitted to produce semaglutide preparations, and telehealth companies have built substantial businesses around this pathway. As of mid-2026, branded Ozempic and Wegovy supply has largely stabilized, though regional and dose-specific shortages still occur. Off-label Ozempic prescribing for weight loss has been criticized for diverting supply from diabetic patients who need the drug for glycemic control, and the ethical dimension of this debate is real.
How to talk to your doctor about Ozempic for weight loss
Walking into an appointment and asking for Ozempic by name often doesn’t go well. Physicians hear this request dozens of times a week now, and many have developed a practiced script in response. The conversation goes better when you approach it as a medical discussion rather than a product request.
Start with your weight history. Before you mention any medication, lay out the timeline. How long have you been at your current weight? What have you tried , specific diets, exercise programs, commercial weight-loss programs, previous medications? When did each attempt start and end, and what happened? Physicians are trained to assess weight as a chronic, relapsing condition, and documenting failed lifestyle interventions builds the case that pharmacotherapy is appropriate rather than premature.
Bring numbers, not anecdotes. Walk in with your BMI calculated, your most recent blood pressure reading, and any lab results you have , lipid panel, fasting glucose, HbA1c, liver enzymes. If you have sleep apnea, joint pain, or other weight-related comorbidities, have those diagnoses documented. The clinical criteria that guide prescribing , BMI ≥ 30, or BMI ≥ 27 with comorbidities , are objective, and meeting them strengthens your position considerably.
Acknowledge the off-label issue directly. If you have diabetes, Ozempic is on-label and the conversation is straightforward. If you don’t, acknowledge that you understand Ozempic’s FDA indication is for type 2 diabetes and that you’re asking about off-label use. Ask whether Wegovy might be more appropriate given your insurance situation. A physician who hears you understand the regulatory field is more likely to engage substantively than one who hears a TikTok-informed demand.
Be prepared for a “no.” Some physicians will not prescribe Ozempic off-label under any circumstances, and their reasons are often institutional: health system policies, malpractice concerns, or personal discomfort with the practice. If you encounter this, ask about alternatives , Wegovy, referral to an obesity medicine specialist, or enrollment in a clinical trial. A refusal to prescribe Ozempic doesn’t have to end the weight-management conversation.
Insurance Coverage: the diabetes diagnosis problem
The single biggest barrier to getting Ozempic for weight loss is not finding a willing prescriber , it’s getting insurance to pay for it.
How prior authorization works against you. When a pharmacy submits an Ozempic claim without a type 2 diabetes diagnosis code attached, the claim often rejects automatically at the point of sale. If your doctor submits a prior authorization, the insurer reviews your chart for evidence that you meet their coverage criteria , which, for Ozempic, typically requires an HbA1c ≥ 6.5% or an existing diabetes diagnosis confirmed by lab work. If your A1c is normal (below 5.7%), the prior authorization will likely be denied regardless of your BMI. The system is binary, and non-diabetic patients fall on the wrong side of the gate.
The Wegovy alternative. If your insurance plan covers weight-loss medications , and roughly 60% of large employer plans now do, up from about 45% in 2020 , Wegovy is the on-label option. Prior authorization for Wegovy typically requires documented obesity (BMI ≥ 30) or overweight with comorbidity, plus evidence of previous lifestyle intervention attempts. The approval rate for Wegovy among plans that cover it is substantially higher than for off-label Ozempic, because the diagnosis code matches the FDA label.
Medicare’s weight-loss drug prohibition. Medicare Part D is statutorily prohibited from covering medications “when used for weight loss.” This prohibition, enacted as part of the Medicare Modernization Act of 2003, has become increasingly contentious as the evidence base for GLP-1 agonists in obesity has strengthened. The Treat and Reduce Obesity Act, reintroduced in multiple congressional sessions, would amend this prohibition, but as of mid-2026 it has not passed. For Medicare beneficiaries without diabetes, branded semaglutide is effectively unavailable unless you pay cash.
Cash-pay options and manufacturer savings programs. Novo Nordisk offers a savings card for Wegovy that can reduce the monthly cost to approximately $650–850 for commercially insured patients whose plans do not cover the medication. For Ozempic, a similar program exists but is restricted to patients with a type 2 diabetes diagnosis. Compounded semaglutide from licensed compounding pharmacies can cost $200–400 per month, though the FDA has warned about quality inconsistencies and has explicitly stated that compounded semaglutide is not FDA-approved.
Alternatives if you can’t get Ozempic
If off-label Ozempic isn’t accessible , whether because your doctor won’t prescribe, your insurance won’t cover, or the cost is prohibitive , you still have options that are grounded in clinical evidence.
Wegovy (semaglutide 2.4 mg). The most direct alternative is the same drug in its FDA-approved obesity formulation. If your insurance covers weight-loss medications, Wegovy is usually the easier prior authorization. The weight-loss results are equivalent to or slightly better than off-label Ozempic at 2.0 mg, because 2.4 mg is a 20% higher dose. The downside is cost if insurance doesn’t cover it.
Zepbound (tirzepatide). Eli Lilly’s dual GIP/GLP-1 receptor agonist, approved for chronic weight management as Zepbound, produces mean weight loss of approximately 21% in non-diabetic populations , meaningfully more than semaglutide’s 15%. In the SURMOUNT-5 head-to-head trial, tirzepatide produced 47% more weight loss than semaglutide. If your insurance covers Zepbound and your goal is maximum weight loss, the data favors tirzepatide. Availability has improved considerably in 2026 following manufacturing scale-up.
Oral semaglutide (Rybelsus). Novo Nordisk’s oral formulation of semaglutide, approved for type 2 diabetes at doses up to 14 mg daily, has been studied for weight loss in non-diabetic populations. Phase 3 data presented in 2023 showed that oral semaglutide 50 mg daily produced weight loss of approximately 15% at 68 weeks, comparable to injectable semaglutide 2.4 mg. An FDA decision on a weight-loss indication for high-dose oral semaglutide is expected in 2026. For patients who cannot tolerate injections, this represents a potentially important alternative.
Older obesity medications. Phentermine-topiramate (Qsymia), naltrexone-bupropion (Contrave), and liraglutide 3.0 mg (Saxenda) all have FDA approval for weight management and produce more modest results , typically 5–10% weight loss. These may be appropriate for patients with lower baseline BMIs or those who cannot tolerate GLP-1 agonists’ GI side effects.
Metabolic and bariatric surgery. For patients with BMI ≥ 35 with comorbidities or BMI ≥ 40, bariatric surgery remains the most effective intervention for sustained weight loss, producing mean loss of 25–35% of body weight maintained over 5–10 years. The 2022 American Society for Metabolic and Bariatric Surgery guidelines now recommend consideration of surgery for patients with BMI ≥ 30 and type 2 diabetes, reflecting growing recognition that surgical metabolic intervention can produce disease remission. Surgery carries surgical risk , a 0.1–0.5% 30-day mortality rate , but for appropriately selected patients, the risk-benefit ratio is favorable.
Frequently asked questions
Can I take Ozempic if my blood sugar is normal?
Yes , from a clinical perspective, semaglutide stimulates insulin secretion only when glucose is elevated (it’s glucose-dependent), so it does not typically cause hypoglycemia in people with normal blood sugar. The STEP trials enrolled non-diabetic participants with normal fasting glucose and HbA1c, and rates of clinically significant hypoglycemia were extremely low [1]. That said, “can” is not the same as “should,” and the off-label nature of this use requires a physician’s assessment of your individual risk-benefit profile.
Do I need a diabetes diagnosis to get Ozempic?
No , legally, your physician can prescribe Ozempic off-label for weight loss without a diabetes diagnosis. Practically, without that diagnosis on file, insurance will almost certainly deny coverage, and you’ll be paying cash. Some physicians will not prescribe off-label regardless, as a matter of personal or institutional policy.
Is Wegovy the same as Ozempic?
Chemically, yes. Both contain semaglutide as the active ingredient. Wegovy goes to 2.4 mg weekly for weight loss; Ozempic goes to 2.0 mg weekly (maximum) for diabetes. The difference is regulatory labeling, not pharmacology.
Will I regain weight if I stop taking it?
The evidence strongly suggests yes. STEP 4 showed that participants who stopped semaglutide after 20 weeks regained approximately two-thirds of lost weight over the following year [3]. This is consistent with the broader obesity medicine literature: pharmacotherapy for obesity works as long as you take it, and weight regain after discontinuation is the norm, not the exception.
Does semaglutide work better in non-diabetics than diabetics?
On average, yes. STEP 1 (non-diabetic participants) showed 14.9% mean weight loss; STEP 2 (diabetic participants) showed 9.6% on the same 2.4 mg dose [1]. The difference likely reflects underlying metabolic differences, concurrent medications, and disease severity rather than any differential drug effect.
Is it safe to take long-term?
The SELECT trial followed 17,604 non-diabetic participants for a mean of nearly 3.5 years on semaglutide 2.4 mg, and the safety profile remained consistent with what shorter trials showed , predominantly GI side effects, no new safety signals, and a 20% reduction in major adverse cardiovascular events [5]. For longer-duration data, we’re still waiting, but the available evidence supports a favorable safety profile for chronic use in appropriately selected patients.
References
Wilding JPH, Batterham RL, Calanna S, et al. “Once-Weekly Semaglutide in Adults with Overweight or Obesity.” New England Journal of Medicine. 2021;384(11):989–1002. PMID: 33567185
Wadden TA, Bailey TS, Billings LK, et al. “Effect of Subcutaneous Semaglutide vs Placebo as an Adjunct to Intensive Behavioral Therapy on Body Weight in Adults With Overweight or Obesity: The STEP 3 Randomized Clinical Trial.” JAMA. 2021;325(14):1403–1413. PMID: 33625476
Rubino D, Abrahamsson N, Davies M, et al. “Effect of Continued Weekly Subcutaneous Semaglutide vs Placebo on Weight Loss Maintenance in Adults With Overweight or Obesity: The STEP 4 Randomized Clinical Trial.” JAMA. 2021;325(14):1414–1425. PMID: 33755728
Rubino DM, Greenway FL, Khalid U, et al. “Effect of Weekly Subcutaneous Semaglutide vs Daily Liraglutide on Body Weight in Adults With Overweight or Obesity Without Diabetes: The STEP 8 Randomized Clinical Trial.” JAMA. 2022;327(2):138–150. PMID: 35015037
Lincoff AM, Brown-Frandsen K, Colhoun HM, et al. “Semaglutide and Cardiovascular Outcomes in Obesity without Diabetes.” New England Journal of Medicine. 2023;389(24):2221–2232. PMID: 37952131
“Efficacy and safety of semaglutide in non-diabetic adults with overweight or obesity: A meta-analysis of randomized controlled trials.” European Journal of Pharmacology. 2026. PMID: 41580006